BROKEN FOREARM
(RADIUS or GALEAZZI FRACTURE)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: ulnar fracture (another type of broken forearm); children's broken forearm (both bone forearm fracture); radial head fracture (type of broken elbow); broken wrist; broken elbow; broken arm; swollen elbow
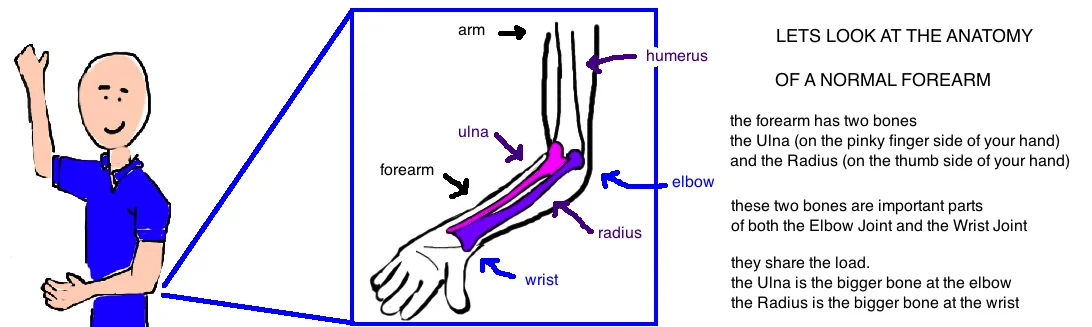
What is a Forearm Fracture of the Radius?
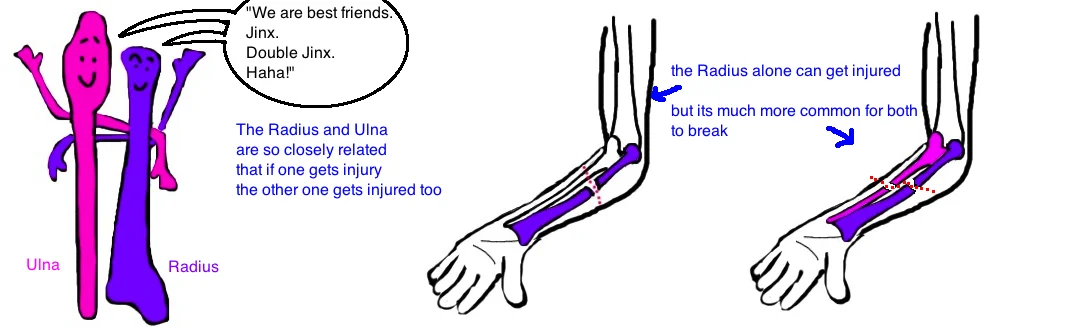
Your forearm has two bones. The Radius is one of your forearm bones (the other is the ulna). It got its the name "Radius" because thats latin for "spoke" like the spokes of a bicycle tire, and this bone rotates around the other forearm bone (the Ulna) like when you twist your wrist when turning a doorknob. The radius is the main forearm bone to form the wrist joint (it meets up with other wrist bones). But as you move toward the elbow, the radius gets thinner and smaller as the ulna becomes bigger, so that at the elbow, the ulna makes up the larger portion of the elbow joint. The two forearm bones work together closely, so its typical for both to be injured during an accident (and important to look for injury to the other bone, even when just one appears injured).
Its common for the radius to be injured by itself (the ulna is ok) near the wrist joint. This is called a distal radius fracture (see talk), and its the most common type of broken wrist. In this talk we look at Broken Forearms (same bone, different location). In the forearm the Radius and Ulna are so closely connected, that when the Radius breaks in the middle, the ulna is almost always injured too.
In kids, a fracture of the radius and ulna is called a "both bone forearm fracture" (see talk).
A Galeazzi Fracture is a specific pattern of injury to the radius and ulna that is commonly seen in adults. It usually occurs when someone falls onto an outstretched hand or receives a direct blow to the forearm, like in a car accident. In a Galeazzi Fracture, the radius bone breaks near the wrist (the 1/3 of the bone closest to the wrist), and the ulna bone is actually dislocated at the wrist. This DRUJ is normally held together by ligaments on the front and back of the wrist, these ligaments can tear when too much force is imparted into the wrist (for more info on DRUJ injuries, see talk).
How is a Forearm Fracture of the Radius diagnosed?
A broken forearm or a Galeazzi Fracture is first suspected by listening to the history of a person's injury and their symptoms. People report wrist and forearm pain, with swelling and possibly a bent forearm (it just doesnt look straight).
Doctors will get X-rays of the wrist and forearm to definitively diagnose the injury. Basic x-rays will show the broken Radius. Remember, that whenever you see a radial shaft fracture near the wrist, doctors will be suspicious for a DRUJ injury. The DRUJ injury is difficult to identify on x-ray because this is a dislocation (an injury to the wrist joint), not a broken bone, and therefore there wont be a clear fracture on x-ray. It requires careful examination to see if there is too much space between the radius and ulna at the wrist, or if the ulnar styloid (tip of the ulna bone) is broken, or if the ulna has shifted backward (dorsal) in the wrist. These findings all suggest that the ligaments which hold the DRUJ together have been damaged. However, to complicate things a little, the ligaments can also be damaged without showing any of the signs we just mentioned, and thus the only diagnose this injury would be with an MRI, or by testing the stability once someone is sedated (because it can be painful).
How is a Forearm Fracture of the Radius treated?
Treatment is different for kids and adults.
In kids, most of the both bones forearm fractures and the isolated radius fractures can be treated successfully without surgery because a kid's bones are young and still growing, and they will heal very well. The injury can be fixed by re-aligning the bones usually while the child is sedated (put to sleep with medicines). A splint or cast is used to hold the forearm in alignment while the bone heals over the next few weeks.
In adults, its a different story.
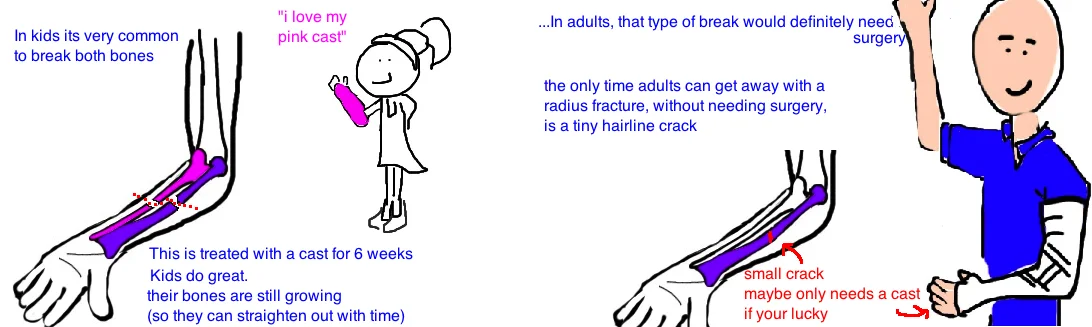
An isolated radial shaft fracture almost always requires surgery. If theres just a hairline crack in the radius and the bone is perfectly aligned then a cast may be the only treatment required (the goal of all fracture care in orthopedics is to obtain and maintain good alignment. If the bone is already aligned, then alignment needs to be maintained by protecting the bone).
In most other cases surgery is recommended, even if the bone is just a little bent. Remember that this bone must rotate around the ulna to allow us to perform daily functions like turning a doorknob or opening a jar or using toilet paper. Any alteration to the angle of the bone will lead to dysfunction of our forearm. The broken radius bone will be repaired with a plate and screws, with attention made to restore (or just maintain) the shape of the bone.
In a Galeazzi fracture, the radius is fixed with a plate and screws, while the DRUJ is repaired with a few pins that get removed after 4 weeks. The pins hold the joint in the correct position while the torn ligaments have time to heal.
What is the long term outcome?
If the injury is healed with the bones in proper alignment, patients recover very well and return to their pre-injury mobility. However, failing to restore normal alignment causes limitations in forearm function.
Reference
Radial Shaft Fracture
1) Hughston JC. Fractures of the distal radial shaft, mistakes in management. JBJS 1957; 39: 249-64. full article. poor outcome with nonop rx radius fx, high nonunion rate.
2) Anderson LD et al. Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. JBJS 1975; 57: 287. full article. 193 radial fx 98% union rate.
3) Hertel R et al. Plate osteosynthesis of diaphyseal fractures of the radius and ulna. Injury 1996; 27: 545-548. full article. more recent article looking at same as above. also high union rate with orif.
4) Schemitsch EH et al. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. JBJS 1992; 74: 1068-78. full article. must restore radial bow wihtin 5 degrees normal or lose 20% rotation.
Galeazzi Fracture
1) Galeazzi R. Uber ein besonderes syndrom bei verletzungen im bereich der unterarmknochen. Arch Ortho Unfallchir 1934; 35: 557-62. original description of injury in 18 pts in milan italy.
2) Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg 2010; 35: 1870-7. full article. great paper on historical evolution of treatment approach.
3) Hughston JC. Fractures of the forearm: anatomical considerations. JBJS 1962; 44: 1664-67. full article. 35/38 conservative treated failed. highlights need for orif.
4) Mikic ZD. Galeazzi fracture-dislocations. JBJS 1975; 57: 1071-1080. full article. looks at 125 pts, highest number, shows orif + k-wire of druj works, first to suggest need for k-wire.
5) Rettig ME, Raskin KB. Galeazzi fracture-dislocation: a new treatment-oriented classification. J Hand Surg 2001; 26: 228-235. full article. >50% of radius fx within 7.5 cm of DRUJ were unstable, req. k-wire, while only 1/18 >7.5 cm were unstable. recommends orif, then testing druj stability. pin if unstable. if druj irreducible, then open to remove tissue, then pin.