MENISCUS TEAR
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
What is a Meniscus Tear?
A meniscus tear is the most common reason for someone to undergo knee surgery (arthroscopic surgery).
The meniscus is a cushion that runs along the border of our knee joint. It works with our cartilage as a shock absorber when we are walking and running. The meniscus bears about 50% of our body weight when walking. Thats a lot of responsibility for a spongy piece of tissue. If the meniscus is damaged, people develop knee arthritis at an earlier age because so much extra force is transmitted to the cartilage. In people that completely lose their meniscus, 20% will develop significant arthritis in just 3 years, and 100% develop significant arthritis in 20 years.
Each knee has two menisci, an inner (medial) and an outer (lateral) meniscus. The medial meniscus tears more commonly (except during an ACL tear when the lateral meniscus tears). In the elderly population its common to see degenerative changes to the meniscus in the back of the knee (its so common that doctors consider this a part of the natural aging process and will not consider surgical treatment unless there are extenuating circumstances).

How is a Meniscus Tear diagnosed?
A meniscus is typically torn when the knee is abnormally twisted. After the injury patients will complain of knee pain, localized to either the inner or outer side of the knee, and often describe an unusual sensation, like having “cotton” inside of the knee.
In some cases, the knee will catch and lock while walking, which occurs because the torn meniscus is getting caught between the bones and preventing knee motion. This finding strongly suggests a meniscus tear, however, it does not occur with all tears. In the office, your doctor will perform a McMurray’s test, which attempts to cause this symptom, thus giving a clearer picture of whats going on inside the knee.
The knee may get swollen after a meniscal tear, however it doesn’t blow up like a balloon as seen in ACL tears (see talk). Doctors will typically order an x-ray to make sure there are no fractures causing the knee pain, however the meniscus is only visualized by MRI.
An MRI is the best test for diagnosing a tear. It will not only show the tear, it allows doctors to assess its severity so that your surgeon can decide on the best treatment.


How is a Meniscus Tear treated?
A meniscus tear can be successfully treated with or without surgery.
Nonsurgical treatment is ideally suited in cases of small tears which are minimally to moderately painful, and lack mechanical symptoms (no locking). The classic RICE (Rest, Ice, Compress, Elevate) is effective at treating the pain and swelling. Most meniscal injuries improve with time.
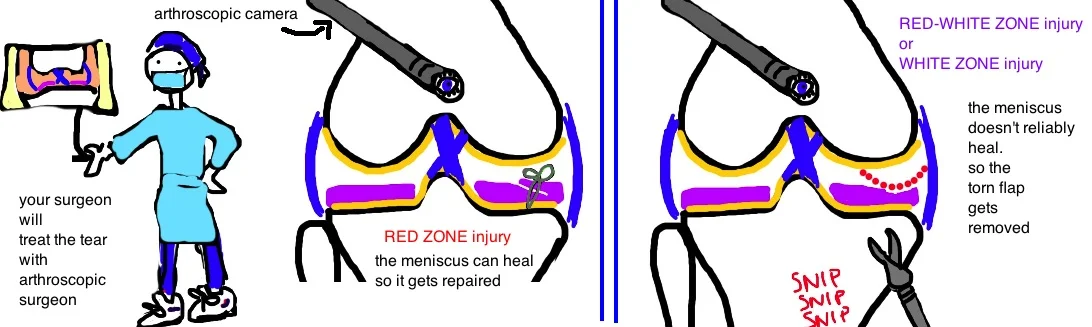
In cases of more severe injury, particularly those that cause limitation in knee motion, surgery can effectively treat symptoms. The torn portion of meniscus is either removed or repaired depending on its location. Remember that healing of bone and all other tissue depends on blood supply (blood delivers the nutrients needed for healing, so areas with good blood supply heal well). The meniscus has great blood supply at its outer rim, however the blood supply disappears as you go toward the center of the knee. Thus there is a red zone (good blood supply), a red-white zone (ok blood supply) and a white zone (poor blood supply). Different zones get different surgery.
The red zone can be repaired because it has good blood supply. Your surgeon will make two or three small incisions around the knee and arthroscopically (camera and instruments) suture the tear back together. There is a high success rate with the procedure.
In contrast, tears in the red-white or white zone don’t heal well because they have poor blood supply, and so surgeons will arthroscopically “clean up” the torn meniscus (read: remove the injured tissue to prevent it from causing pain and mechanical problems). The short term success of the procedure is about 80%, however, patients face an increase risk for early arthritis if an excessive amount of meniscus is removed. This risk depends on the severity of the tear (in fact, risk for arthritis is probably related more to the initial injury than to the amount of meniscus removed with surgery).


What is the long term outcome?
Meniscal tears are effectively treated with both surgery and nonsurgical methods.
In surgical treatment, a meniscal repair is ideal, although not always possible because of the variable blood supply to the injured region. Most patients respond well to the initial surgery, however, some studies indicate that long-term risk for early arthritis may not be easily prevented.
There is a lot of research going into meniscus reconstruction using manufactured biomaterials. There are some products available for use, however, the long-term outcome (over 10 years) is not available because it hasn’t been on the market long enough. Early results show some issues with re-tears, and implant instability, however, with ever improving technology there is a bright future for the application of biomaterials in meniscal tear treatment.
References
1. Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med 1982; 10: 90-95. full article. blood supply.
2. Ahmed AM, Burke DL. In-vitro measurements of static pressure distribution in synovial joints: Part I. Tibial surface of the knee. J Biomech Eng 1983; 105: 216-225. full article. 50% load transmitted through meniscus in 90 deg flex, >50% in ext via hoop stress transmitted to horn of meniscus, loss of meniscus dec contact area by 50% inc contact pressure.
3. Fairbank TJ. Knee joint changes after meniscectomy. JBJS Br 1948; 30: 664-70. full article. first paper to show arthritis postmeniscetomy.
4. Cooper DE et al. Meniscal repair. Clin Sports Med 1991; 10: 529-48. full article. describe zones and radial vs. longitudinal tear.
5. Karachalios T et al. Diagnostic accuracy of a new clinical test (the Thessaly test) for early detection of meniscal tears. JBJS 2005; 87: 955-962. full article. McMurry only 50% sensitive, 90% specific (click with varus/valgus stress + IR/ER). Thessaly test, on one leg at 20 deg flex + IR/ER, has 89% sensitive, 95% specific.
6. Bernthal NM et al. Can the reparability of meniscal tears be predicted with MRI? Am J Sports Med 2011; 39: 506-10. full article. mri only 71% sensitive in detecting tear, cannot determine if reparable vs. partial menisectomy.
7. Scott GA et al. Combined posterior incision and arthroscopic intra-articular repair of the meniscus: an examination of factors affecting healing. JBJS 1986; 68: 847-61. full article. heals within 2 mm of rim, over 4 mm has high failure. tear length <1 cm is stable and doesnt req. repair, >4 cm is so unstable it will probably fail. radial tear usually extends in avascular zone-req. partial menisectomy. horizontal tear is degenerative. longitudinal tear best to repair.
8. Noyes FR et al. Arthroscopic repair of meniscal tears extending into the avascular zone in patients younger than twenty eyars of age. Am J Sports Med 2002; 30: 589-600. full article. successful healing of avascular zone.
9. Allaire R et al. Biomechanical consquences of a tear of the posterior root of the medial meniscus: similar to total meniscectomy. JBJS 2008; 90: 1992-31. full article. lost hoop tension prevents shock absorptive fxn. lateral meniscus tear occurs during ACL injury, medial meniscus tear occurs from ACL deficiency.
10. Noyes FR et al. Meniscus repair and transplantation: a comprehensive update. J Orthop Sports Phys Ther 2012; 42: 274-90. full article. postop rehab routine. 4-6 wks weight bear in extension, passive flex, then begin strengthen.
11. Grant JA et al. Comparison of inside-out and all-inside techniques for the repair of isolated meniscal tears: a systematic review. Am J Sports Med 2012; 40: 459-68. full article. 15% failure rate.
12. Arthroscopic meniscal repair: analysis of treatment failures. Bach BR Jr, Dennis M, Balin J, Hayden J. J Knee Surg. 2005 Oct;18(4):278-84.