DDH
(Developmental Dysplasia of the Hip)
(" Hip Dysplasia ")
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently.
What is DDH (Developmental Dysplasia of the Hip)?
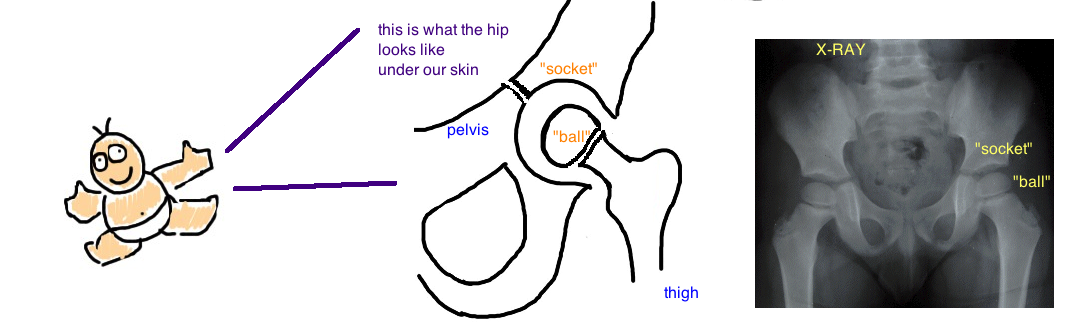
Developmental dysplasia of the hip (called "DDH") is a condition mostly seen in newborns and infants, where the hip has an abnormal shape (the ball and socket don't match up perfectly, like a square peg trying to fit in a round hole...but not quite this different). Dysplasia is a medical term for "abnormal shape", and in DDH the abnormal shape leads to increased risk of hip dislocation and abnormal growth.
What causes DDH? Its a type of "packaging disorder". Packaging disorders occur during pregnancy when the fetus is squished ("packaged" too tightly within the uterus) and causes abnormal bending of the arms or legs. Packaging disorders are more common in female babies (they naturally have more lax ligaments), a mother's first child (because the uterus is tighter), gestational diabetes and other conditions that cause the fetus to be too big or the amount of fluid surrounding the baby to be too little. Other packaging disorders include torticollis (wry-neck, see talk) and metatarsus adductus (see talk).
In pregnancy, the ball and socket of the hip must be in close contact because they grow together and model each other to fit perfectly. If theres a packaging issues, the ball and socket of the hip joint arent in close connection so as the pregnancy progresses the hip grows more abnormally and becomes unstable (the hip can dislocate).


How is DDH (Developmental Dysplasia of the Hip) diagnosed?
Every newborn baby is examined for hip stability because DDH is not uncommon and it can be successfully treated if detected and treated early in childhood.
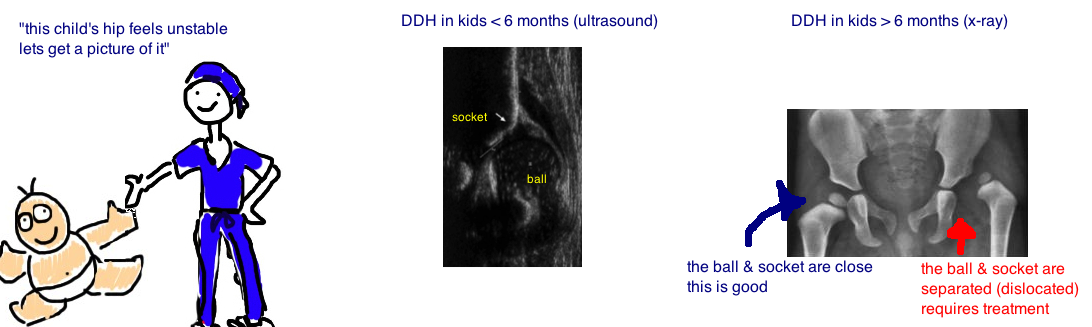
The hip instability is tested by stressing the hip with the Barlow Test (a doctor attempts to dislocate the hip), and the Ortolani Test (the hip is dislocated and the doctor attempts to re-locate the hip). If there is concern for hip instability further tests (imaging studies) are ordered so doctors can look at the hip.
If the child is less than 6 months old (which is most common), then ultrasound is used to look at the hip. If the child is older than 6 months, then x-ray is used to look at the hip. The reason for this difference is that the "ball" portion of the hip isnt fully covered in calcium until 6 months, and so it cannot be seen on x-ray until 6 months, so ultrasound must be used. The position of the "ball" and the shape of the "socket" are measured to determine if there is DDH, and if so, how severe.

How is DDH (Developmental Dysplasia of the Hip) treated?
Once DDH is diagnosed, it is treated based on the severity and the age that its diagnosed.
Age is very important because the younger the baby the easier it is to correct. Newborns and infants are very plastic, meaning their bones havent hardened yet and so they can be molded easily, while calcium slowly enters the bone and hardens it as we get older.
A Pavlik harness is used to treat DDH in kids under 6 months old whose hip stays in place (the ball is inside the socket, but it can dislocate if the hip is stressed too much). The harness holds the hip in a position thats stable, so it wont dislocate. During the time that a child wears a Pavlik harness, the ball and socket stay in contact so the hip gets molded into a stable shape. However, the Pavlik harness doesnt always work, sometimes the hip is just too unstable.
A spica cast (which covers the pelvis, hips and legs) is used to treat DDH in kids under 6 months old who are too unstable to rely on a Pavlik harness. A spica cast does the same thing as a Pavlik harness (it holds the hip in a position that keeps the ball and socket together), but its much more stable than a Pavlik harness. A spica cast is also used to treat kids 6 - 18 months old (too old to benefit from a Pavlik harness).
Whether a Pavlik harness or spica cast is used, kids are treated this way for a few months to give the bone and surrounding soft tissue time to settle in this better position.


Unfortunately, sometimes nonoperative treatment isnt enough to create a stable hip. Surgery is required in cases of DDH that remain unstable despite attempts to keep the hip stable with a Pavlik harness and spica cast. Its also required in kids older than 18 months because their hips have slowed in their growth by this point and doctors cant rely on the body's ability remodel the hip.
Surgery will reshape the ball portion or the socket portion (depending on the location of abnormal shape). The "ball" is typically reshaped with a "Varus Osteotomy" which drives the "ball" medially into the socket. The "socket" is typically reshaped with a "Pelvic Osteotomy" (either a Pemberton,Degas, or Salter if the triradiate cartilage is open; or a salvage if teh triradiate is closed). The Pelvic Osteotomy extends the socket outward (lateral) to give more coverage over the "ball". Sometimes both the ball and socket are reshaped, sometimes only one needs to be reshaped.
What is the long term outcome?
Kids do best when the condition is treated early in life. Our bones are the most pliable when we are infants, so our bones can be molded into a good position (even if they start out in a bad position)... but as we get older our bones become hard and cannot be re-shaped. Think of our bones like wet-clay right after birth, but as we get older the bones turn into hard-clay and cannot be shaped.
The most challenging cases occur when the child is older and surgery is required to reshape the ball and socket. The amount of surgery required to correct DDH becomes progressively greater with increasing age. And what if the ball and socket are not reshaped... there is an increased risk of hip arthritis because of abnormal contact stress in the hip. This means increased risk of arthritis at an earlier age, however, not all kids with an abnormal hip get arthritis, and not all kids that get arthritis (as seen on x-ray) feel hip pain as a result. There is a lot of debate among doctors about whether its worth intervening with surgery at a young age, or just waiting until the child becomes an adult, let them have a normal childhood, before considering hip surgery.
DID WE ANSWER YOUR QUESTIONS? IF NOT, PLEASE EMAIL US: contact@bonetalks.com
Reference
1) Zamzam MM et al. Acetabular cartilaginous angle: a new method for predicting acetabular development in developmental dysplasia of the hip in children between 2 and 18 months of age. J Ped Ortho 2008; 28: 518-23. full article. outcome measure acetabular remodel after closed reduction.
2) Mladenov K et al. Natural history of hips with borderline acetabular index and acetabular dysplasia in infants. J Ped Ortho 2002. 22: 607-12. full article.
3) Carsi B et al. Incomplete periacetabular acetabuloplasty. Acta Ortho 2014; 85: 66-70. full article.