BROKEN COLLAR BONE (CLAVICLE FRACTURE)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: broken shoulder (proximal humerus fracture); separated shoulder (AC joint); shoulder dislocation; shoulder instability; broken arm (humeral shaft fracture); rotator cuff tear
What is a Broken Collar Bone (clavicle fracture)?
The collar bone, also known as the clavicle, is a commonly broken bone, especially in active younger people.
The collar bone breaks when someone falls onto an outstretched arm, and the force of this fall gets transmitted up the arm to the collar bone. Less commonly, it breaks from a direct blow (the collar bone protected only by very thin covering of soft tissue - you can easily feel the bone under the skin).
In a healthy person, our collar bone supports the shoulder joint as a person raises their arm above their head. In fact, if the clavicle is frozen, you cannot raise your arm much beyond shoulder height. The clavicle also keeps all the muscles that move your shoulder under the right amount of tension.
How is a Broken Collar Bone (clavicle fracture) diagnosed?
Doctors are suspicious for an injury to the collar bone when people report a traumatic event and complain of tenderness over the collar bone and pain when moving their shoulder.
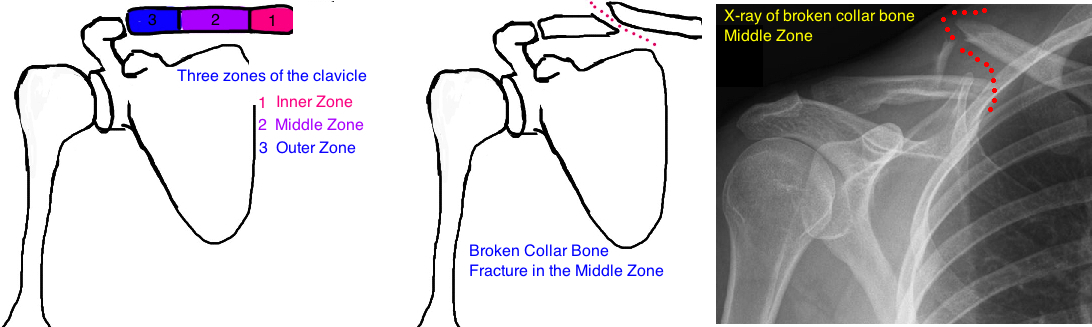
X-rays are ordered and x-ray alone is sufficient to diagnose the injury. CT scans and MRIs are not needed.
When thinking about clavicle fractures the bone gets separated into thirds. The inner third, the middle third and the outer third. Doctors will classify the break as an inner, middle or outer third fracture.
How is a Broken Collar Bone (clavicle fracture) treated?
Treatment is based on the location (zone 1, 2, or 3) and the severity of the break.
The vast majority (80%) occur in the middle of the collar bone (Zone 2). And most of these can be treated with just a sling to provide comfort - no surgery necessary. The bone heals slowly over time - the broken ends become "sticky" and this allows the ends to reconnect, and new bone surrounds the broken ends to form a single .

But some breaks may benefit from surgery. Surgery is recommended when doctors are concerned that the bone will not heal ("nonunion" which is when the broken ends fail to re-unite).
There are a few risk factors for nonunion. If the collar bone has broken and become completely displaced (the two ends of bone don’t line up), or if the two ends overlap by more than 2 cm, there is about a 15% risk of a nonunion. There is also an increased risk in females, the elderly (people over 60 years old), and breaks that have many small fragments (also called a "comminuted fractures").
So why is a "nonunion" such a big deal? Its a big deal because many people will continue to feel pain in their collar bone. They will actually feel the two ends moving around. You may also feel that your shoulder doesnt have the same strength it used to... or it may get tired more easily. To some people, especially very active people, this may be unacceptable. In this case some surgeons recommend re-connecting the bone ends with a metal plate and screws. By realigning the bones and holding them in place there is a 98% chance the bone will heal (nothing in medicine is 100% guaranteed). But remember that theres no free lunch in medicine, and surgery has its own risks and complications, such as injury the nerves that provide sensation to the skin over the collar bone. Also, because there is so little soft tissue covering the collar bone, you can often feel the metal under your skin and this can be irritating - around 25% of people who get surgery, will get a second surgery to remove the irritating plate and screws. Lastly you will have a scar from surgery.
Its important to note that even with a nonunion, a lot of people will not complain of any problems and will go about their daily activity problem-free. So nonunion does not mean you automatically get surgery, it just means there is a higher tendency for lasting discomfort.
Ultimately, the question is whether its worth taking someone for surgery when they have an 85% chance of healing very well, and over 90% chance of being asymptomatic.
It’s a conversation to have with your doctor about your expectations. Some people will initially wait and see how well the bone heals, and if they continue to experience symptoms many weeks after their injury, then they decide to get surgery. Waiting a few weeks has not been shown to affect the success of surgery.
There are some situations where surgery strongly strongly recommended: 1) if the bone pokes through the skin (open, or "compound" fracture), 2) if the bone fragment is pushing strongly against the skin (this is "skin tenting" and eventually the bone will erode through the skin and become an open fracture); 3) if there are additional fractures to the shoulder; or 4) if the person injures a nerve or artery due to the fracture.
Other than these circumstances, the benefit of surgery is debated.
What is the long term outcome?
People with injuries to their clavicle sometimes complain of decreased shoulder motion and pain if it does not heal with normal or near normal alignment. With that said most clavicles heal very well and there are no long term problems with pain or function.
Sometimes a small bump in the bone will remain after the break has healed. This is like a scar after a bad cut on your skin. Your body heals the injury, and adds scar tissue to add strength to the site of injury to prevent future problems.
References
1) Khan LA et al. Fractures of the clavicle. JBJS 2009; 91: 447-60. full article. review of all clavicle fx.
Middle 1/3 Fractures
2) Zlowodzki M et al. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. JOT 2005; 19: 504-7. full article. this paper started re-examination of surgical benefits for this injury.15% risk nonunion with risk factors: displaced,comminuted, female, elderly. reduced nonunion with orif.
3) Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. JBJS 2007. 89; 1-10. full article. landmark study. 15% nonunion with displaced clavicle, only 20% of those are painful. orif improves nonunion rate, but 30% complication, 18% req. reoperation usually for removal hardware.
4) Robinson CM et al. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. JBJS 2013; 95: 1576-84. full article. orif vs. nonop displaced fx: better constant/dash score (due to better union rate), increase complications.
5) Potter JM et al. Does delay matter? The restoration of objectively measured shoulder strength and patient-oriented outcome after immediate fixation versus delayed reconstruction of displaced midshaft fractures of the clavicle. J Shoulder Elbow Surg 2007; 16: 514-8. full article. no difference in acute vs. delayed orif, so ok to wait to see if nonunion develops.
6) McKee MD et al. Midshaft malunions of the clavicle. JBJS 2003; 85: 790-7. full article. orif/oseotomy of malunion is successful.
7) Vander Have KL et al. Operative versus nonoperative treatment of midshaft clavicle fractures in adolescents. JPO 2010; 30: 307-312. full article. clavicles in kids: all fx healed but 20% painful malunion. 16 vs. 12 weeks return to activity.
8) Andersen K et al. Treatment of clavicular fractures. Figure of eight bandage versus a simple sling. Acta Ortho Scand 1987; 58: 71-4. full article. nonop rx: equal outcome but sling more comfortable.
9) Collinge C et al. Anterior-inferior plate fixation of middle-third fractures and nonunions of the clavicle. JOT 2006; 20: 680-6.. full article. orif anterior plate has fewer complications.
Outer 1/3
10) Banerjee R et al. Management of distal clavicle fractures. JAAOS 2011; 19: 392-401. full article. review.
11) Oh JH et al. Treatment of distal clavicle fracture: a systematic review of treatment modalities in 425 fractures. Arch Ortho Trauma Surg 2011; 131: 525-33. full article. all technique equal effect on union, but hook plate has most complications.