"PINCHED NERVE" IN THE LOW BACK - HERNIATED DISK
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
What is a Lumbar Disk Herniation?
A lumbar disk herniation causes back pain and neurologic symptoms by compressing a spinal nerve.
A disk herniation is an abnormal out-pouching of a vertebral disk. The disk is a cushion between two vertebrae (aka spine bones).
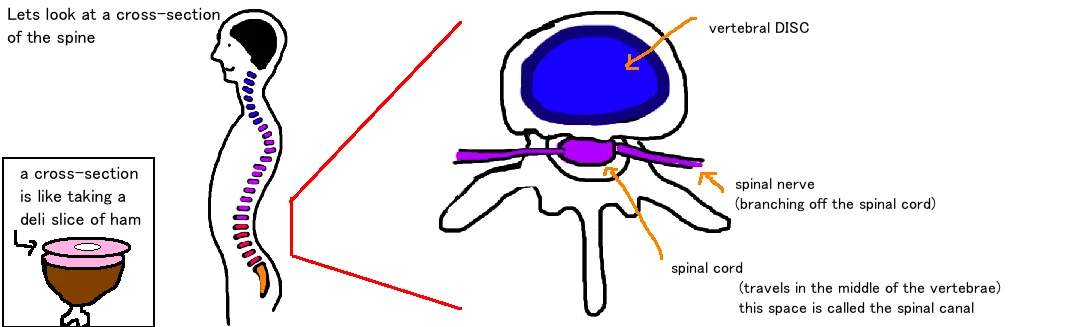
Lets quickly review the anatomy of the spine to better understand how a disk herniation causes pain.
A disk lives between each of the vertebrae and acts as a squishy shock absorber and enables motion between your vertebrae (this is what allows you to twist at your hips…if the vertebrae were just one long bone you would be as inflexible as a lead pipe). Each disk is named after the two vertebrae that it sits between. For example the disk at L4-L5 sits between the 4th and 5th lumbar vertebrae.

The disk is like a jelly doughnut, a squish fluid inside with a slightly firmer outer shell which holds everything together. The "jelly" is called the nucleus pulposis and its 80% water, but starts to dry out in your 30s and continues to dry out the rest of your life. As it becomes more dehydrated, the disk loses its height and becomes less resilient to absorbing shock. When the disk receives a shock too strong to fully absorb, the inner "jelly" squirts out (aka Herniates) and causes back pain by pushing on the near by spinal nerve.
The nerve that gets "pinched" is called a spinal nerve. Spinal nerves brach off the spinal cord at every level of the spine. Our spinal cord is the mother of all nerves and it travels from your brain to your lower back. It travels through the center of your spine. The spine is made of many vertebrae (spine bones) that are stacked on top of each other, and held together by ligaments. As the spinal nerves branch off, they exit the spine through small holes in our vertebrae called foramen, and then travel to our arms and legs.
The problem is that these spaces (the foramen) are narrow. Anything that causes the space to get even smaller can compress the nerve and cause pain. One thing that causes this space to get smaller is a disk herniation.
About 95% of all lumbar disk herniations occur at levels L4-L5 and L5-S1.

How is a Lumbar Disk Herniation diagnosed?
A person with a pinched nerve in their back reports pain starting in their low back and radiating down their leg. They often will also complain of some numbness or weakness in the same leg (its typically just one leg thats affected, unlike spinal stenosis).
About 90% of people have pain, about 60% have numbness and 40% have weakness. There are other things that cause back pain and these conditions need to be considered before diagnosing a herniated disk. The disk itself has pain sensors, and a worn out disk (without any herniation) is a separate type of pain called discogenic pain (see talk). Spinal stenosis can also cause pain radiating down the leg (see talk).
The location of the pain and/or numbness within the leg can be used to determine which of the spinal nerves is being pinched. If theres a hernia in the disk between L4 and L5, it can affect the L4 nerve if its compressing at the foramen and lateral recess, and the L5 nerve if its compressing in the paracentral region (which is much more common: about 95% of the time).
If a patient is lying down and their leg (the one with pain) is lifted off the floor, it will create tension on the nerve, and this will often make the pain much worse if the nerve is truly being pinched. This is the "straight leg test". Patients often complain of pain while sitting (their back is arched forward) and relief when standing up right (this is the opposite as people with spinal stenosis).
X-rays of the back are important to look at the architecture of the vertebral bones, and to make sure they are all correctly stacked on top of each other, like blocks. If not, and one bone has slid forward, this is a separate condition called spondylolisthesis (see talk), which is the cause of a similar pain but requires a different treatment. X-rays can show bone but dont show soft tissue (like your disks or your nerves).
An MRI however is great at showing soft tissue and swelling. MRI is an important test to look for compression of the spinal nerves, and is frequently ordered if symptoms don’t improve after 6 weeks, or if symptoms occurred after a trauma (like a car accident). The MRI is very sensitive for identifying abnormal spines, however its oftentimes too sensitive. Only 5% of disk herniations between L4-5 or L5-S1 actually cause pain. Its therefore important to confirm the MRI findings with the area of pain or numbness, which muscles are weak, and this makes sure you are treating the true problem. Surgery on a “bulging disk” that’s not actually compressing the nerve will not help with pain.
A sudden and dramatic change in neurologic function, or a sudden numbness in the groin region, or an inability to control your bowel or bladder movements suggests a syndrome called “cauda equina” which is more serious and considered an emergency because those symptoms may not improve if not treated quickly.
How is a Lumbar Disk Herniation treated?
Treatment should proceed in a stepwise fashion from least invasion methods to more invasive if pain persists.
The good news is that low back pain from a pinched nerve typically gets better with time. Studies show that in 90% of people, symptoms get better within the first 90 days. During this time people are encouraged to initially rest and then slowly increase activity as tolerated. Physical therapy is recommended. Anti-inflammatory medications are effective in treating pain, oftentimes muscle relaxants are helpful to treat spasms (although they can make people very drowsy). A steroid dose pack is another option that is given to reduce inflammation. Overall, treatment with anti-inflammatories and treatment with surgery has about the same outcome results at 4 years.

Epidural or nerve root injections have also been shown to effectively treat herniated disks, specifically helping with pain and providing long lasting treatment in about 50% of patients (compared to 90% with surgery).
Surgery is indicated for patients with severe pain and disability for more than 6 weeks after trying to treat the pain with the methods described above.
The surgery is called a discectomy and laminectomy. Pressure on the pinched nerve is relieved by removing some of the herniated disk, and removing some of the bone (the lamina). Studies show surgery very effective in reducing pain, but less effective (about 50/50) at allowing for neurologic recovery. Patients that have pain radiating down one leg, and an obvious hernia on MRI have better surgical outcomes.

What is the long term outcome?
Non-surgical treatment helps with most cases lower back herniated disks, because over time our body absorbs the “jelly” that was pinching the nerve. Our body is adaptive and smart and can often decompress itself. But some cases require surgery because the nerve is being pinched so significantly that nothing is going to change that until a surgeon goes in creates a bigger space for the nerve to live. Surgery can permanently improve symptoms of pain and will prevent the progression of this disorder.
Questions? Email us: contact@bonetalks.com