SHOULDER INSTABILITY (TORN LABRUM)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: shoulder dislocation; broken shoulder (proximal humerus fracture); separated shoulder (AC joint); broken arm (humeral shaft fracture); rotator cuff tear
What is Shoulder Instability?
There are two types of shoulder instability.
1) A traumatic injury (usually after a shoulder dislocation, see talk) will cause uni-directional instability (unstable in one direction: the arm bone usually wants to dislocate out the front of the shoulder).
2) Then there is multi-directional instability which results from chronic overuse of the shoulder (common in butterfly swimmers) or in people with naturally lax joints. In this case, the arm wants to dislocate (or partially dislocate, this is called subluxation) any way it can.
Before we talk about how the shoulder becomes unstable, we must first talk about how the shoulder normally remains stable. The shoulder has an incredible range of motion (yet the bone itself moves less than 1 mm from the joint center at the far arch of motion). Move your shoulder around and you see its more flexible than any other joint, which is great for activities. But theres pros and cons to everything, and as your body enables increased flexibility, your body is sacrificing stability. In fact the shoulder dislocates more commonly than any other joint. Our shoulder is a ball and socket joint where the arm bone (humerus) is the ball that fits into the glenoid (a part of the shoulder blade, "scapula"). It actually looks like a golf ball sitting on a tee (and for you golfers, think about how easy it is for a golf ball to fall off the tee... just a light breeze). The shoulder tries to compensate for the lack of stability by relying on muscles (like the rotator cuff) and soft tissue (like the labrum, and ligaments) to provide additional stability.
The labrum surrounds the "socket" to increase the depth of the joint. There are also a lot of ligaments to hold the joint together. The most important is the Inferior ligament (IGHL), which prevents forward (anterior) translation, and the Middle ligament (MGHL) which also blocks forward translation. Lastly the Superior ligament blocks inferior translation (stops the arm bone from falling into your armpit). The joint also is surround by a capsule which gives stability. Last but not least, there are the rotator cuff muscles, the deltoid, the biceps, and the pec muscle which all help with stability. The muscles keep the joint stable during normal range of motion, while the ligaments and capsule keep everything in place in the extremes of motion - like when your arms are bent all the way back in a swan dive.
Now that we understand stability. Lets look at the cause of and solution for shoulder instability.
1) What is Unidirectional Instability (labral tear)?
Unidirectional instability occurs after a traumatic event (typically a shoulder dislocation) and in 95% of cases the shoulder is unstable anteriorly (the arm wants to fall out the front of the joint). The shoulder injury will tear the soft tissue stabilizers of the shoulder, and these will not heal without surgery. The inferior ligament-labrum-joint capsule complex is the most commonly injured structure. With this soft tissue torn, theres nothing holding the arm bone within the joint during sharp movements.
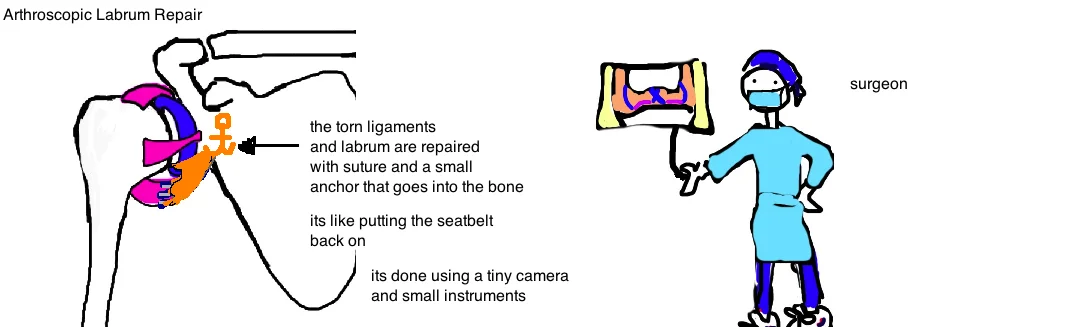
Think of the soft tissue as a seat-belt. In most cases a seatbelt isnt critical for keeping the driver inside the car, however, during an accident, if theres no seatbelt then theres nothing to stop the driver from going out of the car. The same is true for these ligaments. The arm wont be constantly falling out of the joint, but during a sharp movement, or a minor fall, theres no seatbelt, and this is when the arm will pop out.
How is Unidirectional Instability (labral tear) diagnosed?
Diagnosis of instability starts with a person reporting an injury to their shoulder and subsequent feelings of shoulder looseness. People feel like the shoulder is shifting around (they may also report that its dislocated one or more times).
A doctor will test stability with the "Apprehension Test". This test puts a force on the shoulder, provoking it to dislocate out the front, and the doctor sees how "apprehensive" the patient feels about the whole thing. Haha. I know it sounds pretty mean spirited, but its a very accurate way to test instability.
If injury to the labrum and ligaments is suspected, then an MRI is ordered (an x-ray is really best for seeing bone fractures, but cannot show injury to these ligaments). Sometimes, if the injury is old, and there is scarring inside the shoulder, then tears are harder to see and an MRI arthrogram is used (this means an MRI is done after a contrast fluid is injected into the shoulder joint). This will reveal subtle tears of the capsule and ligaments.
How is Unidirectional Instability (labral tear) treated?
Treatment can be nonsurgical or surgical.
Nonsurgical treatment uses physical therapy to strengthen the muscles that are still healthy, which can be trained to provide more stability to the shoulder and compensate for some of the lost stability. However, full compensation is not possible and many people will still report instability (and many experience additional dislocations).

In such cases, surgery can effectively repair the damaged soft tissue (a labrum repair and joint capsuleplication) using arthroscopic techniques (a camera and mini-tools).
After surgery, the arm is kept in a sling for 3 weeks to allow for healing. Rehab is then progressed to passive motion (pendulum exercises) and some forward flexion, external rotation, abduction by 6 weeks. Muscle strengthening begins at 9-12 weeks. People are expected to return to full activity after the surgery (although the most common complaint is some shoulder stiffness: remember stiffness is stability, and in this case your surgeon has decided to sacrifice a small amount of motion, to prevent a future dislocation).
The rare case of unidirectional posterior instability occurs in athletes like offensive linemen in football, and some pitchers (where repeated stress of the arm bone pushing against the back of the shoulder joint causes laxity).
2) What is Multidirectional Instability?
Multidirectional instability is associated with shoulder laxity and feelings that the shoulder will dislocate, without any history of a traumatic event that started the instability. Its associated with long-time overuse of the shoulder, like in swimmers. This instability often occurs in both shoulders.
Treatment for multidirectional instability: It responds very well to rehabilitation and strengthen exercises, which often needs to be done for 6-12 months. The key is to strengthen the rotator cuff muscles, and the peri-scapular muscles which all work together to stabilize the shoulder. If rehab fails, then surgeries to tighten the capsule (capsule plication) are often successful.
Questions? Contact@bonetalks.com
REFERENCES
1. Arthroscopic Bankart repair versus nonoperative treatment for acute, initial anterior shoulder dislocations. Arciero RA, Wheeler JH, Ryan JB, McBride JT.
Am J Sports Med. 1994 Sep-Oct;22(5):589-94
Hovelius L, Olofsson A, Sandström B, Augustini BG, Krantz L, Fredin H, Tillander B, Skoglund U, Salomonsson B, Nowak J, Sennerby U. JBJS 2008 May;90(5):945-52
3. Recurrent posterior shoulder instability. Robinson CM, Aderinto J. J Bone Joint Surg Am. 2005 Apr;87(4):883-92.
4. Treatment of the athlete with multidirectional shoulder instability. Levine WN, Prickett WD, Prymka M, Yamaguchi K. Orthop Clin North Am. 2001 Jul;32(3):475-84
5. Imaging techniques for the evaluation of glenohumeral instability. Sanders TG, Morrison WB, Miller MD. Am J Sports Med. 2000 May-Jun;28(3):414-34.
6. A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Sanders TG, Miller MD. Am J Sports Med. 2005 Jul;33(7):1088-105
7. Arthroscopic capsulolabral reconstruction for posterior instability of the shoulder: a prospective study of 100 shoulders. Bradley JP, Baker CL, Kline AJ, Armfield DR, Chhabra A. Am J Sports Med. 2006 Jul;34(7):1061-71.
8. Posterior labral injury in contact athletes. Mair SD, Zarzour RH, Speer KP. Am J Sports Med. 1998 Nov-Dec;26(6):753-8.
9.
10.