LESSER TOE DEFORMITIES
(Hammertoe, Claw Toe, Mallet Toe)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: big toe deformity; plantar plate rupture; achilles tendon rupture; flat foot; charcot foot
What are Lesser Toe Deformities?
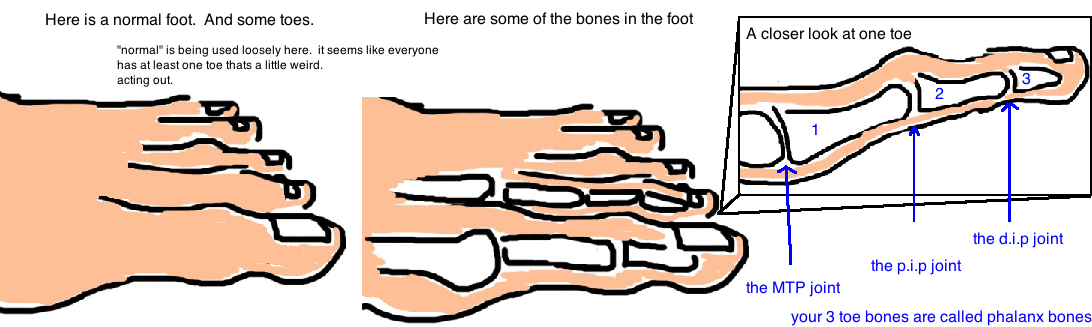
Sometimes our toes can get twisted or bent out of shape. Our toes are made of small bones that are held together by small tendons and even smaller ligaments. These can become loose or tear over time, which allows toes to become malaligned.
While there are many types of toe deformities, the claw toe, hammertoe and mallet toe are the most common and will be described here.
What is a Claw-toe?
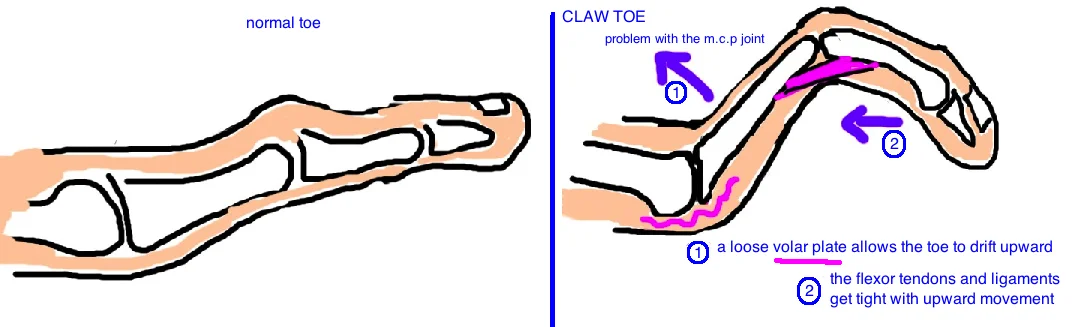
A claw toe occurs at the MTP joint (metatarsophalangeal joint). The volar plate (a thick piece of tissue at the bottom of our foot) normally provides stability to this joint but it can become loose over time due to joint inflammation (synovitis) or can be torn if a toe is bent backward during an injury (see turf toe). Additionally, this deformity is commonly seen in children or adolescents with the neuromuscular disease Charcot-Marie-Tooth. In all cases, the toe slowly drifts upward which causes the tendons at the bottom of the toe to become tight. These tight tendons then pull the rest of the toe downward, making the toe curl.
Diagnoses is made by examining the toe. X-rays are often ordered to also look at the bone alignment. Patients are tender at the bottom of their foot, at the MTP joint. This occurs because the change in joint alignment causes a bony prominence which will rub against the ground.
Treatment depends on the severity of pain and the severity of the deformity. Initially, treatment consists of providing orthotics or insoles to decrease the pressure over the affected toe. Even though this does not correct the appearance of the toe, it can prevent pain and may patients only want to avoid a painful foot.
If a patient wants to correct the toe’s appearance, then surgery is required. If the toe is out of position but loose enough to straighten out, then surgery can be performed to rebalance the tendons to keep the toe straight. If the toe is stuck in the curled position, then the tendons are rebalanced, and the joint itself is removed and the toe is repositioned into correct alignment.
The toes are pinned in position for 4-6 weeks while the toe heals. Overall there is a high cure rate with this condition (whether patients elect shoe modification or surgery) although there is always a risk of recurrence, or a risk that surgery is overly aggressive and the toe becomes unstable and just “flops” around (called a "floating toe").
What is a Hammertoe?

A hammertoe is a toe deformity that occurs at the P.I.P joint (proximal interphalangeal joint). The extensor tendon that attaches here (over the top of the foot) is too tight, and so it pulls the toe upward into a prominent position. This is a problem because this joint will rub against the toe-box of most shoes causing painful “corns” to develop. The neighboring MTP joint may be slightly extended but its not the major site of deformity (otherwise, its considered a claw toe). However, a loose MTP joint (like a floating toe from a plantar plate injury, see talk) is often associated with a hammertoe, and it should be evaluated whenever a hammertoe is seen.
The diagnosis consists of looking at the toe and seeing the deformity. X-rays are often ordered to look for other associated injuries, like MTP instability.
Treatment depends on how irritating the toe becomes. Patients can try shoes with bigger toe-boxes so theres no rubbing over the toe, or a gel sleeve can be placed over the toe to prevent friction.
If patients want the toe deformity to be corrected, then surgery is needed. If the toe is flexible, then the tendons can be rebalanced (flexor to extensor) to straighten the toe. If the toe is rigid in the hammer position, then the joint is removed (proximal phalanx head resection), sometimes the joint is fused, and the soft tissue is rebalanced. The toes are pinned in position for 4-6 weeks while the toe heals. Overall patients do very well.
What is a Mallet toe?
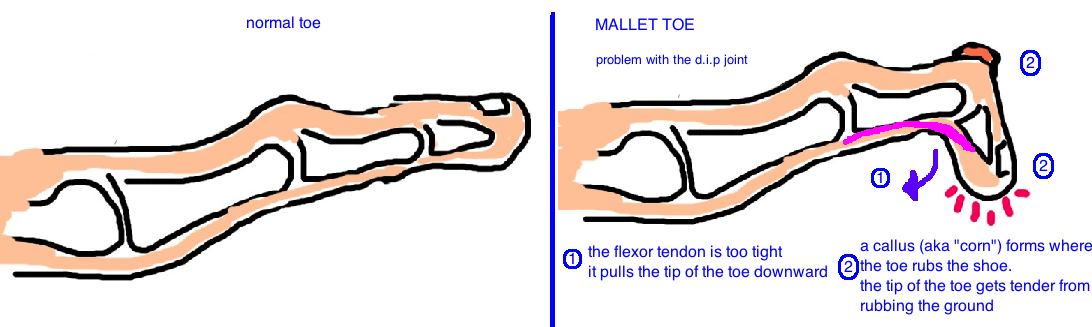
A mallet toe is a deformity that occurs at the D.I.P joint (distal interphalangeal joint). It is caused by a tendon imbalance. The flexor tendon becomes contracted (tightened) and this pulls the tip of the toe downward.
The diagnosis is made by looking at the toe and seeing the deformity. Patients often complain of pain at the tip of the toe because its pushed into the ground with each step.
Treatment, like the other toe deformities, depends on the amount of toe pain and a person's expectations.
You can try wider shoes that better accommodate this deformity or use a little gel cushion to pad the tips of the toe to prevent or minimize callus formation. The goal is to take pressure off the affected area.
The alternative is to undergo surgery to rebalance the tendons. The surgery to correct the deformity is similar to the surgeries required for a claw or hammer toe. If the toe is still flexible, then the tight tendon can be released/loosened, or if the toe is stiff, then the tendon is released and the joint itself is removed. The toes are pinned in position for 4-6 weeks while the toe heals. People do very well with the procedure, with about 95% of people being satisfied with the treatment.
Reference
1) Dhukaram V et al. Correction of hammer toe with an extended release of the metatarsophalangeal joint. JBJS Br 2002; 84: 986-90. full article.
2) Coughlin MJ et al. Operative repair of the fixed hammertoe deformity. Foot Ankle Int 2000; 21: 94-104. full article. fusion vs. fibrous nonunion equal outcome, 85% satisfaction; 92% pain relief.
3) Coughlin MJ. Operative repair of the mallet toe deformity. Foot Ankle Int 1995; 16: 109-116. full article. 95% success with dip resection or fusion. only 75% fuse but fibrous nonunion doesnt matter.
4) Boyer ML, DeOrio JK. Transfer of the flexor digitorum longus for the correction of lesser-toe deformities. Foot Ankle Int 2007; 28: 422-430. full article. effective rx hammer toe to reduce metatarsalgia, corn, but only 50% completely resolves.
5) Shirzad K et al. Lesser toe deformities. JAAOS 2011; 19: 505-14. full article. review.