ROTATOR CUFF TEAR
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: rotator cuff arthritis; shoulder dislocation; labral tear of shoulder; biceps tendon rupture
What is a Rotator Cuff Tear?
A Rotator Cuff Tear can occur after a single sports injury (an acute tear), or it can occur after years of wear and tear (chronic degenerative tear). We will talk about both.
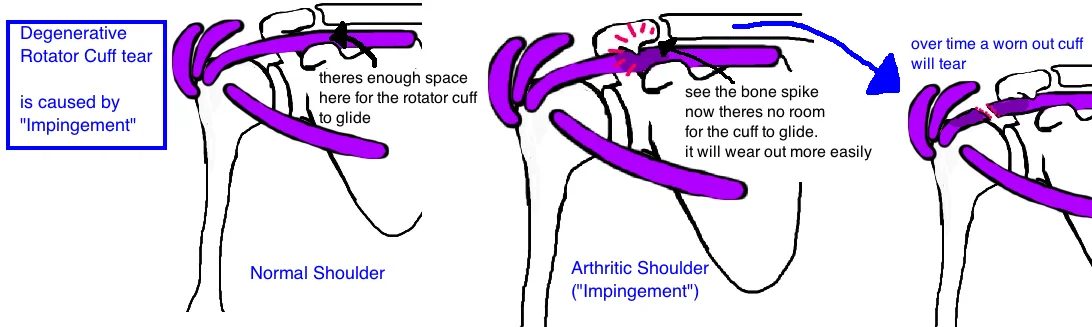
The slow degenerative type is the most common. A chronic rotator cuff tear, and Shoulder Impingement Syndrome are part of a broader spectrum of shoulder disease. The space in our shoulder that holds the rotator cuff gets narrower (this is impingement) with age. This narrowing causes the rotator cuff to rub along the bones of our shoulder, and all this friction creates small tears in the cuff. Overtime these partial tears can develop into full tears.
The process can occur at earlier ages in laborers or active people due to "overuse" (not all active people develop this condition). This type of rotator cuff tear (also called rotator cuff degeneration) is the most common type.
An acute tear (a tear after a single event) usually occurs in the middle age or the elderly population after a fall. It can also occur in a younger athlete during a sports related injury. But overall an acute rotator cuff tear much less common than a tear that occurs after decades of wear and tear.
Lets quickly review of the anatomy of our shoulder to understand the rotator cuff.
The Rotator Cuff is actually 4 shoulder muscles that originate along the shoulder blade (scapula) and then come together in the shoulder and insert onto the arm (humeral head). The four muscles are: 1) the supraspinatous, 2) the infraspinatous, 3) the teres minor, and 4) the subscapularis. The rotator cuff kind of looks the inside of a baseball. The biceps tendon (think Popeye) is also closely associated with rotator cuff in the shoulder, and is sometimes referred to as the 5th rotator cuff muscle. The rotator cuff acts to balance and stabilize the shoulder through its range of motion, while the deltoid actually provides the major strength to the shoulder.
How is a Rotator Cuff tear diagnosed?
Doctors are tipped off whether the injury is chronic or acute by the patient's story (was there a specific event that started all the problems? or did things just start happening slowly over time?)
The main symptoms of a Rotator Cuff tear and Impingement is pain (especially at night). People with this problem also commonly report shoulder fatigue, muscle weakness, and sometimes “catching” or "clicking" during arm movement.
Many of us are walking around with minor tears, known as a subclinical injury: meaning its not significant enough to produce symptoms (if a tree falls in the woods, does anyone care?). About 50% of people over 60 had at least a partial tear, while only 4% between 20-30 had a tear, indicating that some degree of degeneration of the rotator cuff is probably a natural part of aging.

Small tears are usually stable (not getting bigger) if there are no symptoms of pain etc. However, if new symptoms (like pain) arise, this may indicate that a small tear is getting bigger.
Significant pain is usually an indication to get an MRI (but first x-rays of the shoulder should be taken to make sure there arent other issues causing this pain).
An x-ray is important to rule out other injuries, however, an MRI is the best test to look specifically for a rotator cuff tear. The MRI is also used to stage the severity of a tear (which helps to determine the best treatment).
Its also important to recognize that many other shoulder injuries can imitate a rotator cuff tear, and so a thorough examination of the shoulder needs to be performed to ensure you're treating the correct thing. SLAP tears, Biceps tendonitis, and a frozen shoulder are all causes of shoulder pain that can be mistaken for a cuff tear.
How is a Rotator Cuff tear treated?
Rotator cuff tears are not all treated the same way because there are a few important things to consider before deciding on a treatment.
Acute tears, experienced by athletes and younger people are typically treated more aggressively (with surgery), as compared to the degenerative tears seen in elderly people.
In part this is because degenerative tears are seen as part of the normal aging process, and surgery cannot reverse the changes of our aging bodies. So even if you fix the tear, theres a high chance the cuff will retear.
Surgical and non-surgical treatment is an option for both groups, but understanding the cause of injury, and future expectations is critical for helping people balance the risks and benefits of treatment options.
Nonoperative treatment for degenerative tears is all about physical therapy. Stretching and strengthening, as well as modification of activity. Stretching will improve posterior capsule mobility, which is critical for motion, while strengthening will recruit surrounding muscles to compensate for the weak cuff.
Even patients that decide to get surgery will need some physical therapy first. Surgical treatment will not work well if the shoulder is stiff beforehand (because surgery will cause a little stiffness due to inflammation), and therefore the shoulder should be flexible before surgery.
If pain persists despite physical therapy, then an arthroscopic evaluation can be performed (a tiny camera is put into your shoulder, so the surgeon can look around).
If the rotator cuff tear is less than 50% thickness (partial tear) then debridement (cleaning) and decompression (shaving down that spike of bone) of the acromion is recommended.
If theres over 50% tear, there a high likelihood of the tear will become 100% (a full tear), and therefore the cuff is repaired (as well as debridement and decompression as seen with partial tears).
What is the long term outcome?
The patients with low functional demands can often be treated successfully with physical therapy alone. Unfortunately, studies have be unable to identify reliable factors (like age, activity level etc) that will predict how quickly the pain will resolve once therapy has begun.
However, some tears will not improve and pain will continue. In such cases surgery can help.
People that undergo surgery typically do well when the post-surgical therapy is followed. Surgery is only the first step on a long road to recovery. Physical therapy is required after surgery to help the shoulder regain its motion and the rotator cuff regain its strength. Physical thearpy isnt started until 2-4 weeks after surgery to allow for the cuff to heal.
References
1) Unruh KP et al. The duration of symptoms does not correlate with rotator cuff tear severity or other patient-related features: a cross-sectional study of patients with atraumatic, full-thickness rotator cuff tears. J Shoulder Elbow Surg 2014; 23: 1052-8.
Questions? Contact@bonetalks.com