Sometimes the ligament-labrum complex will actually tear off a chip of bone from the joint socket (glenoid rim), and this is called a "Bony Bankart Lesion". Sometimes, when the dislocation is very severe, the humeral head gets whacked against the joint socked and causes an indentation, almost like when you press too hard on a ping-pong ball. This is called a "Hill Sachs Lesion". This creates an abnormally shaped "ball" which can easily dislocate from the "socket".
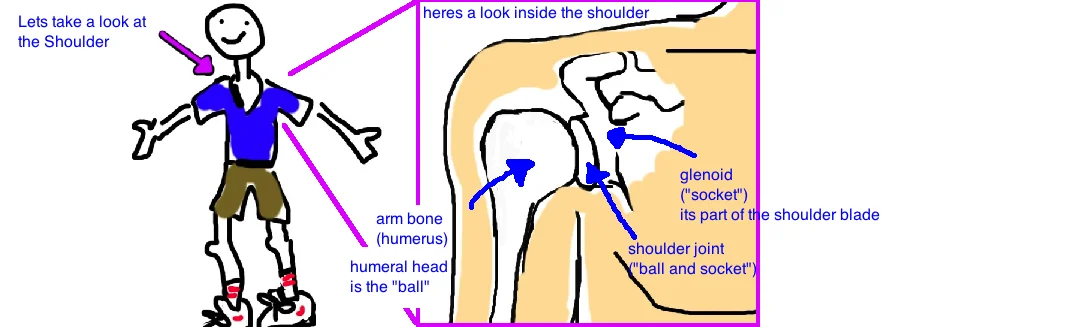
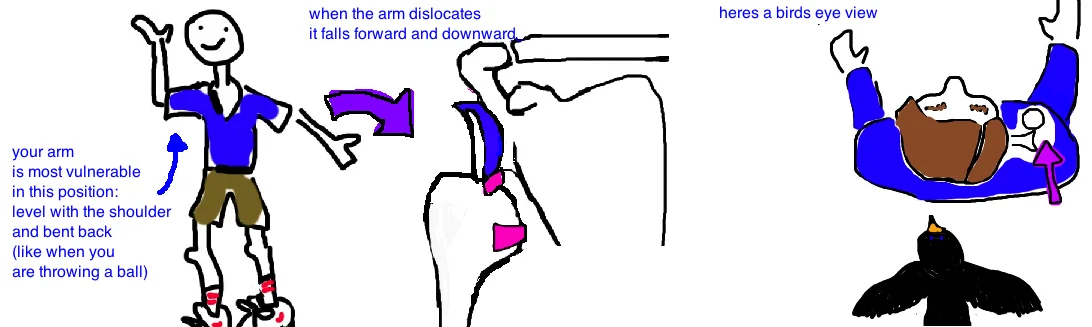
Shoulder dislocations occur in people of all ages and they can be caused in many ways. It most commonly occurs as someone is falling and they grab for something to break their fall. In this position the arm gets forced in a position of abduction (movement away from their body) and external rotation, which causes the arm bone to come forward out of the joint (anteriorly direction). About 95% of shoulders dislocate anteriorly (forward). Posterior dislocations are very rare (the and and are mainly seen in people having seizures, getting electrocuted, or if you are a baseball pitcher with chronic laxity of your posterior joint capsule from the stress of pitching.