KIDS - SCFE
(Slipped Capital Femoral Epiphysis)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently.
What is a SCFE?
A slipped capital femoral epiphysis, or SCFE, is an injury to the hip growth plate in kids.
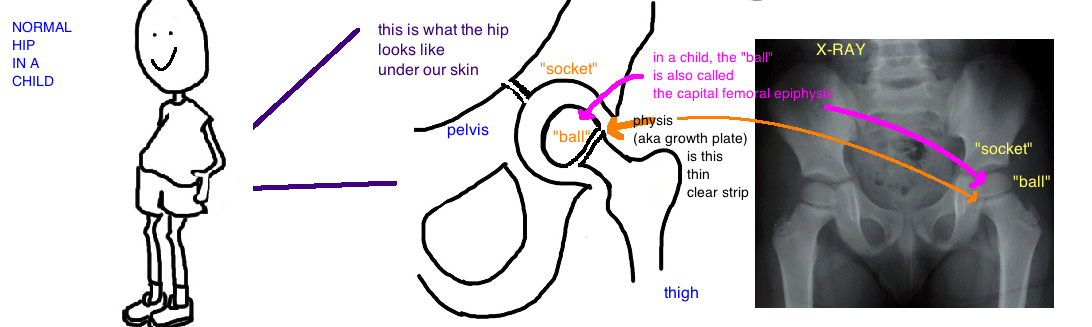
The hip is a “ball-and-socket” joint where your thigh bone (the femur) joins with the pelvis (the acetabulum). The femur is the “ball” while the pelvis is the “socket”. The femur (thigh bone) is made up of a femoral head (which is the ball portion of the hip), and this part is injured in a SCFE.
A SCFE occurs when a weak spot in the growth plate causes the "ball" portion of the hip to slip out of position. The name "slipped capital femoral epiphysis" is a misnomer because the femoral head (aka "capital femoral epiphysis") actually stays in within the hip socket while the femoral neck "slips" forward (aka anterior) and rotates outward (aka external rotation). A SCFE is not a crack in the bone, but more like a crack in the growth plate.

This is a condition that usually occurs in overweight pre-teen males during a period of rapid growth. The rapid growth cases the growth plate to be weak, and it breaks under the weight of the whole body. The disorder usually affects just one hip, however a lot of kids actually experience a slip in both hips (maybe up to 40%). Some conditions increase the risk for both hips to slip, such as endocrine disorders like hypothyroidism and kids receiving growth hormone treatment. If the SCFE occurs before a child is 10 years old, doctors are also more concerned that the other hip will also slip.
Diagnosing a SCFE:
Kids with this injury come into the office with a painful limp. The pain occurs mainly with walking and it radiates into the groin. Kids will also have limited hip motion, especially with internal rotation and abduction.
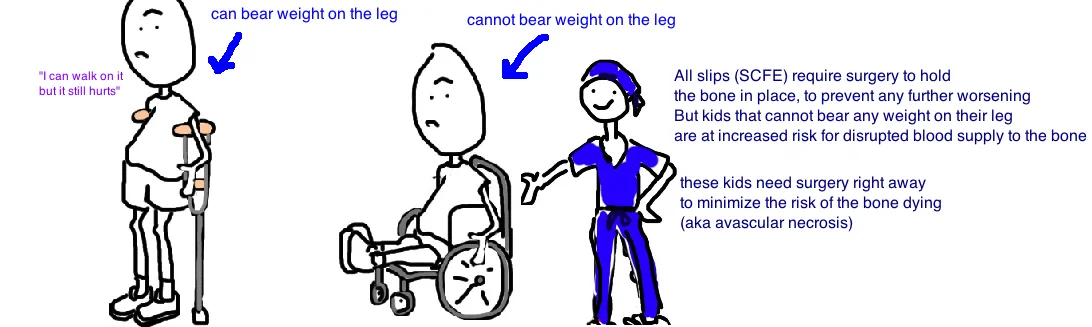
The injury is classified as stable or unstable. Stable means that kids are able to put weight on the affect leg (with or without the aid of crutches), and if kids cannot put any weight on the affected side because of pain, its considered unstable. This distinction is very important because it predicts the risk of complication, and helps doctors decide how urgently to treat the problem.
Pain is a common symptom which alerts parents to this problem, and doctors will take x-rays of the hip, which will confirm the SCFE is the physis has "slipped" out of position. Doctors will draw "Klein's line" on the x-ray to determine if a slip has occurred.
Treating a SCFE:
Treatment for SCFE usually requires surgery. The hip needs to be stabilized to prevent further slip.
To stabilize the hip, a single screw is placed across the growth plate under x-ray guidance to prevent further movement. The surgery is minimally invasive, the incision is usually very small, along the side of the upper thigh. After the surgery kids are allowed only toe-touch weight bearing for 4 weeks to allow the bone to heal, and then they can return to normal activities.

You may be wondering why a slip so bad. There are two reasons why its so bad.
1) A hip with the "ball" portion out of position cannot have normal range of motion, and this may affect athletic performance or basic daily walking.
2) Most importantly, this type of slip can injure the blood supply that provides nutrients to the "ball" portion (femoral head). If this blood supply is injured, it will cause the ball to become weak and collapse. Our bones are more like trees than simple blocks of calcium. Bones have cells that live inside that are constantly repairing the bone and making small changes to strengthen our bone. Our bones need nutrients from our blood for these cells survive, in the same way that a strong tree needs water to survive. A disruption in blood flow causes the hip bone to schrivel up and die (called "avascular necrosis" or "osteonecrosis"). A hip with osteonecrotic bone will be very painful, will progress rapidly to arthritis requiring a hip replacement.

What is the long term outcome?
Overall, when this injury is detected and treated quickly, the outcomes are excellent with >90% of children returning to normal function.
As noted about, the biggest concern with these injuries is the potential for blood flow disruption. A stable SCFE has only a 1-10% risk of injury to the blood supply, while an unstable SCFE has double that risk. Surgery is critical to prevent stable SCFEs from turning into unstable SCFEs, and for preventing unstable SCFEs from progressing even further, and causing high rates of blood supply injury and/or premature arthritis.
DID WE ANSWER YOUR QUESTIONS? IF NOT, PLEASE EMAIL US: contact@bonetalks.com
References
1) Aronsson DD et al. Slipped capital femoral epiphysis: current concepts. JAAOS 2006; 14: 666-79. full article. review.
2) Sankar WN, McPartland TG et al. The unstable slipped capital femoral epiphysis: risk factors for osteonecrosis. J Ped Ortho 2010; 30: 544-8. full article.
3) Loder RT et al. Narrow window of bone age in children with slipped capital femoral epiphyses. J Ped Ortho 1993;13:290-293. full article. epidemiology.
4) Loder RT et al. Acute slipped capital femoral epiphysis: The importance of physeal stability. JBJS 1993;75:1134-1140. full article. stable vs. unstable classification.
5) Matava MJ et al. Knee pain as the initial symptom of slipped capital femoral epiphysis: an analysis of initial presentation and treatment. J Ped Ortho 1999; 19: 455-60. full article. diagnosis of condition.
6) Aronson DD et al. Slipped capital femoral epiphysis: The case for internal fixation in situ. CORR 1992;281:115-122. full article. rx based on xray.
7) Aronson DD, Carlson WE. Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. JBJS 1992;74:810-819. full article. great results stable with one screw.
8) Peterson MD et al. Acute slipped capital femoral epiphysis: The value and safety of urgent manipulative reduction. J Ped Ortho 1997;17:648-654. full article. timing of unstable rx.
9) Beck M et al. Increased intraarticular pressure reduces blood flow to the femoral head. CORR 2004;424:149-152. full article. pressure on hip blood flow.
10) Carney BT et al. Long-term follow-up of slipped capital femoral epiphysis. JBJS 1991;73:667-674. full article. higher complication with nonop rx.
11) Wilson PD et al. Slipped capital femoral epiphysis: An end-result study. JBJS 1965;47:1128-1145. full article. long term outcome f/u good result.
Questions? Email us: contact@bonetalks.com