"PINCHED NERVE" IN THE NECK (CERVICAL RADICULOPATHY)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
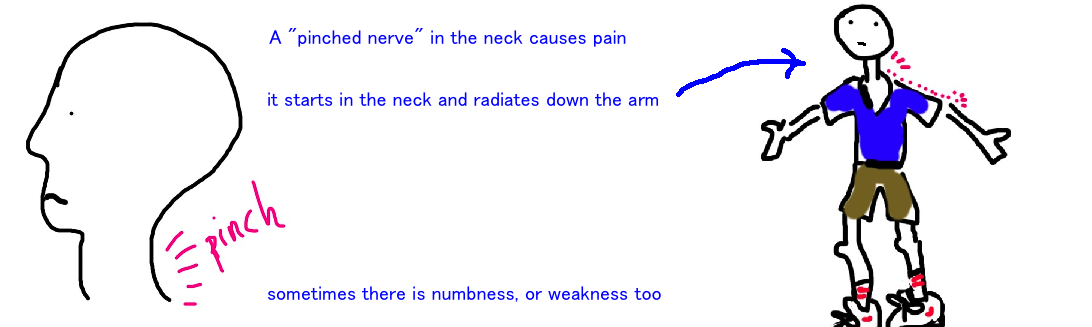
What is a "Pinched Nerve" in the Neck?
Neck pain from a "pinched nerve" refers to injury or irritation of a spinal nerve. The pain usually starts in the neck and radiates into your shoulder or down the arm. This radiating pain is called "radiculopathy".
Before we get too technical lets take a look at the neck and the spine to understand how nerves are at risk for getting injured here.

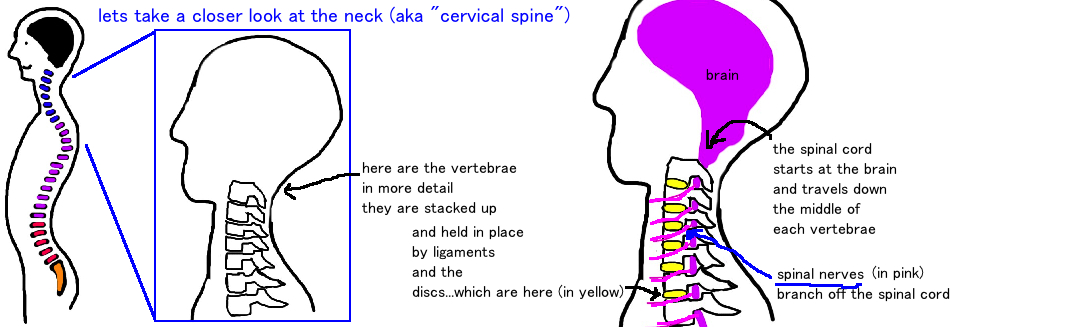

Our spinal cord is the mother of all nerves and it travels from your brain to your lower back. It travels through the center of your spine. The spine is made of many vertebrae (spine bones) that are stacked on top of each other, and held together by ligaments. Spinal nerves are branches off our spinal cord. They branch off at each vertebral level, and then they exit the spine through small holes in our vertebrae called foramen.
The problem is that these spaces (the foramen) are narrow. Anything that causes the space to get even smaller can compress the nerve and cause pain.
There are two major things that can compress the nerve as it exits the spine.
1) The first is a herniated disk. A disk exists between each of the vertebre and acts as a squishy shock absorber and enables motion between your vertebre (this is what allows you to nod your head “yes” and “no”…if the vertebre were just one long bone you would be as inflexible as a lead pipe). The disk is like a jelly donut, a squishy gel-like substance inside (nucleus pulposus) with a slightly firmer outer covering (annulus) which holds everything together. When the disk receives a shock too strong to fully absorb, or if the outer covering gets warn out over time, the middle “jelly” material squirts out and causes neck pain by compressing the nerve that runs right next to the disk.
So our disks are a good thing, until they stop working properly and start causing pain.
2) The other cause of nerve compression is arthritis which causes little bumps to form (osteophytes) which can also press on the nerve (this is stenosis, and this is more commonly seen in the lower back).
Once the nerve is compressed it will cause significant pain in the neck, but also importantly, it will cause pain that radiates down the arm (that follows the course of the nerve from the spinal cord down the arm). Lets look at how its diagnosed in more detail.
How is a Cervical Disk Herniation diagnosed?
A person with a pinched nerve in their neck comes in with pain starting in their neck and radiating down their arm. They often report of some numbness or weakness in the same arm that is having pain.
Remember that nerves both send and receive information. The information nerves send causes our muscles to contract, and if this information is blocked, we feel weakness. Our nerves also receive information in the form of sensation, like temperature, pain, vibration, etc. If this information is blocked, we feel numbness.
Pain caused by spinal nerve impingement will be worsened when someone leans their head back, and rolls it toward the side thats in pain. This is called a Spurlings test. This position decreases the space the nerve travels through and increases its compression, thus worsening the pain.
The location of the pain and/or numbness within the arm can be used to localize which of the 8 cerivcal spinal nerves is being pinched. If there is a herniated disc between C3 and C4, it’s the C4 nerve that gets pinched. The function of the nerves overlap a little, but looking to see where the pain is located can be used to identify which nerve is the culprit.
X-rays of the neck are important to look at the architecture of the vertebral bones, to make sure they are all correctly stacked on top of each other, like blocks. If not, someone may be having a condition called spondylolisthesis (see talk), which is another cause of pain and has a different treatment.
MRI is an important test to look for compression of the spinal nerves. X-rays can show bone but dont show soft tissue (like your disks) unlike an MRI which is great at showing soft tissue and swelling. The MRI is very sensitive for identifying abnormal spines, however its oftentimes too sensitive, and MRIs of people with absolutely no neck pain, still show abnormal disks in about 20% of people.
Its therefore important to confirm the MRI findings with the areas of pain and weakness to make sure you are treating the true problem. Surgery on a “bulging disk” that’s not actually compressing the nerve will not help with pain.
How is a Cervical Disk Herniation treated?
The natural history of neck pain (observing people with neck pain that don’t receive any treatment) has shown that about 75% of cases resolve with time.
One study followed people for 2-19 years after their pain and found that 45% only had one episode of neck pain, 30% continued to have some mild neck pain symptoms, and 25% showed signs of worsening. None of the people developed sudden arm numbness or weakness without a traumatic event, meaning it’s a slow process, there are not quick changes that occur without some type of accident. So while most people get better or have an annoying neck pain that doesn’t majorly disrupt their life, about 25% of people feel like their symptoms are bad enough to require further treatment.
Doctors always start with nonsurgical treatment and try progressively more invasive treatments if the pain fails to resolve.
Physical therapy to strengthen the surrounding muscles is the first treatment. This can help take pressure off the nerves. Also, Anti-inflammatory medications (NSAIDs) help with pain. Some people have also found soft neck collars to help (although theres not evidence in the medical literature to support this) or to use chiropractors to manipulate their backs (there is also no strong evidence to show that this provides significant improvement).
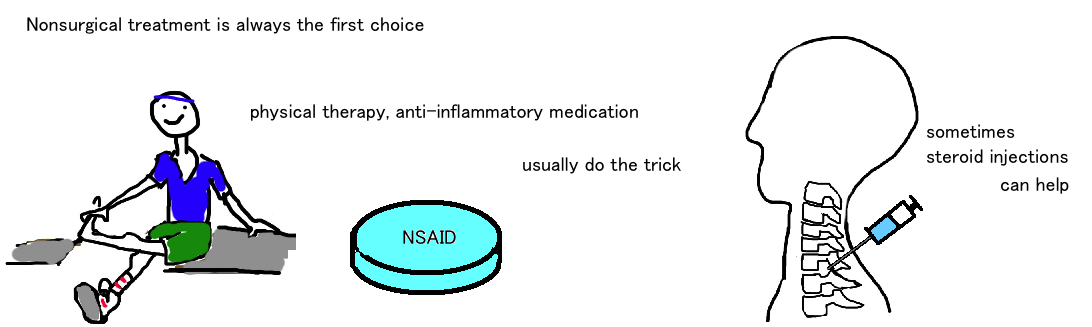
Another popular nonoperative treatment is an epidural injection (where an anti-inflammatory steroid is placed around the inflamed nerve) or a spinal nerve block. There are risks to these procedures (your placing a needle right around the spinal cord and spinal nerves) but some have found the injection very helpful in relieving pain.
If nonoperative treatments have failed to help the pain after 6 weeks at the minimum, or if your neurologic condition is deteriorating (meaning the numbness in your arm is getting worse or your hand keeps feeling numb) then surgery is often the next step.
Surgery to correct neck pain that radiates into the hand has been shown to be very helpful with pain relief in up to 80-90% of cases.
There are two main approaches:
1) from the front of the neck (called an ACDF: anterior cervical discectomy and fusion) The ACDF removes the disk and fills that space with new bone which returns your cervical spine to its normal height and prevents a recurrent herniation from occurring. It fuses the two vertebrae (meaning it creates one bone where there used to be two bones).
2) from the back of the neck (called a laminectomy). The laminectomy removes a piece of bone which is usually not critical for stability of the neck bone, and decompresses the area around nerve. This is a smaller surgery, the bones are not fused, but the disk is not removed and therefore there is a risk that it will herniate again at some later other time.
What is the long term outcome?
The patients typically do great when treated in a stepwise fashion.